


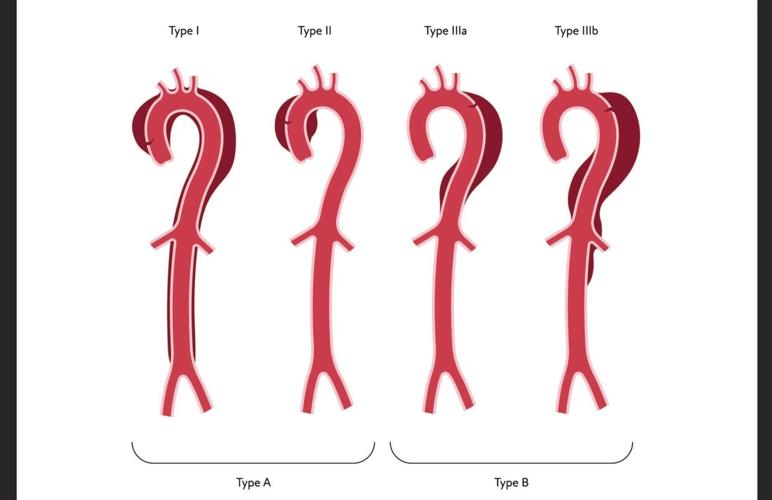
“A type B dissection occurs downstream of all that in the descending thoracic aorta.”
The type of dissection drives the type of treatment. “Both types are very serious problems, and both typically need ICU-level care.”
Type A is an emergency that requires immediate treatment, Zeigler said. “We almost certainly need some kind of operation before the patient goes home with a Type A aortic dissection. Without surgery, half of those patients will die within two days.”
Type B is less likely to cause a rupture. Treatment often involves lowering blood pressure so there is less stress on the aortic wall, followed by stenting to help repair the layers back together. “We are able to treat Type B with stents most of the time,” Zeigler said.
“Both types, after a successful repair, require lifelong monitoring of the remaining segments of the aorta that are dissected. It's impossible for us to treat the whole dissection in one operation most of the time because the aorta is about two-and-a-half feet long.”
People are also reading…
Symptoms
There are symptoms that show up with both types of dissection that people should be aware of, Zeigler said. “The first warning sign can be the severe chest pain, back pain that is the herald of this event happening. But when people say warning signs, they’re usually talking about something that happens a few days ahead of time so they can head it off before it’s a problem.”
Not in the case of aortic dissections. “There’s usually not something like that. Usually, we’re talking about an acute event. If you recognize that there’s a problem and get to a hospital quickly, a hospital can get you triaged and operated on.”
How MUSC is pushing the field forward
While aortic dissections are considered uncommon, they kill an estimated 13,000 Americans each year. So specialists at MUSC are:
- Taking advantage of new technology to help patients. “One of the things we’re very proud of is that we have access to branched stents, which allows us to treat more of these dissections early on while we still have a chance of remodeling the aorta in a positive way,” Zeigler said.
- Enrolling patients in clinical trials testing new devices. “We’re part of clinical trials where we can treat Type A dissections with stents, although that’s very much in its infancy. And we’ve done that in a handful of patients with reasonable results.”
- Studying molecular mechanisms for aneurysm formation and development. “We can potentially prevent these from happening.”
- Identifying patients with a familial cause of dissections and aneurysms. “We treat those patients more aggressively than somebody with a small aneurysm that isn’t ready for surgery.”
- Managing patients through a genetic cardiovascular program. “It helps us care for patients who have syndromic conditions that put them at risk for dissections at a young age, like Marfan syndrome, Ehlers-Danlos or Loeys-Dietz syndrome.”
Going forward
As Zeigler mentioned, doctors are hoping to one day prevent aneurysms and dissections. But they are not at that point yet.
“The current state is that we identify patients who have small aneurysms and watch them over time. And when they reach a certain size threshold, where we think dissection is becoming more likely, then we operate and either do a stent to exclude that aneurysm, or we do open surgery to cut the aneurysm out, depending on its location,” Zeigler said.
“But the reality is there are a lot of patients that are walking around with an aneurysm and don’t know they have one. And there’s a lot of patients that have dissections that didn’t have an aneurysm that we would’ve treated. So there’s some pieces of the puzzle that we still don't have.”













